Mission
Profile
Healthcare Glossary
Healthcare Glossary
Quality, Access, Cost issues frame current day discussions about Healthcare Services. Innovation in today's healthcare arena is manifold: Meaningful Use, Quality Incentives, ACO Development, Digital Records are buzzwords in the current healthcare milieu. Patients, Providers and Insurers are encountering changing CMS regulations, new payment concepts and hybrid delivery models.
The Healthcare Glossary originates with a Business Intelligence perspective and a focus upon research exercises that can be performed internally by a provider. Ideas and concepts are described from an experience perspective melded with data research and policy analysis acumen. Serious issues for today where stakeholders require empirical facts and discovery implicit in cautious, nuanced decision making.
Accountable Care Organizations - An organization managing care and the coordination of patient care services. Provides the patient a seamless approach to the gamut of care services rendered during a treatment episode. The Center for Medicare and Medicaid Services has created a Medicare Shared Savings Program that enhances coordination among providers to improve quality of care and reduce unnecessary costs. An appropriately staffed ACO staffed organizes the myriad care services of a Medicare patient rendered by hospitals, physicians, home care services and other providers. It is a template of a value based purchasing initiative by a governmental insurer. Early estimates by Rand Corporation researchers demonstrated in research prior to the legislation being passed that spending can be slowed and care improved by bundling payments to an ACO entity rather than traditional payments to multiple providers.

A critical path implementation plan is a sine qua non for successful operation. The goals (domains) defined by CMS are fivefold: (1) good care experiences (2) coordination of care services; not readmissions (3) patient safety (4) preventive health (5) managing the health of frail and elderly. It is a risk sharing entity. An ACO coordinates and delivers care to the patient and provides measurement data about that episode to the payer. For a Medicare certified ACO A minimum 5,000 MCARE beneficiaries are enrolled over a three year period. Formations of ACO organizations may by voluntary; perhaps even virtual -- via claim form submissions indicating shared services. Expect Federal Trade Commission analyses that preclude anti-competitive markets seen as inhibiting care delivery innovations that the legislation had intended. Having the analytic tools to monitor utilization and get at root causes are essential. Not achieving good outcomes will expose financial risk. Most importantly the organizational behavior and financial incentives behind accountable care are "here to stay" and inevitably will shape the nature of the care episode in the future.
Adverse Events - Occurrences serious enough to harm a patient during a care encounter. 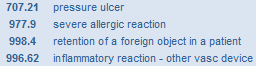 Lowering the occurrence of adverse events is targeted by CMS; it is an integral part of the Value Based Purchasing system planned for October 2012 implementation . Adverse events can include infections, venous thromboembolisms, pressure ulcers, device failures and patients falls. Incentive withholds have gained traction in recent years with private insurers. Although self reporting of harmful events remains problematic, those events, indicated by medical record coding staff within multiple diagnoses categories are located in the extended discharge record (Dx4, Dx5, etc) and become an important data elements for medical management and reimbursement issues.
Lowering the occurrence of adverse events is targeted by CMS; it is an integral part of the Value Based Purchasing system planned for October 2012 implementation . Adverse events can include infections, venous thromboembolisms, pressure ulcers, device failures and patients falls. Incentive withholds have gained traction in recent years with private insurers. Although self reporting of harmful events remains problematic, those events, indicated by medical record coding staff within multiple diagnoses categories are located in the extended discharge record (Dx4, Dx5, etc) and become an important data elements for medical management and reimbursement issues.
Appropriateness - The suitability of a statistic for empirical measurement; it speaks to the cogency of a data element representing a study factor. Although a statistic may be routinely generated to indicate a performance level, the indicator itself may be questioned because of its suitability to the study issue. The transformation culture underway in healthcare delivery and reimbursement initiates a recalibration of performance metrics.
Authorization ñ A de facto approval for providing health services by the insurer. Is an acknowledgement by the HMO insurer (gatekeeper) of the clinical condition, test results and other symptoms that medical intervention is needed: hence reimbursement by the insurer is likely. Accordingly payment denials are sometimes a tacit, albeit ignored, recognition of disagreement among care professionals concerning diagnoses and treatment options.
Benchmark A performance measurement standard. A yardstick to gauge the performance of the health facility's clinical, financial or operational standing. Variances from this norm provide perspective about program strategy and course direction. The norm can be an externally generated indicator (e.g industry reporting) or internally (longitudinal data) reflecting past performances. This statistic is intended to set a empirical marker for measuring performance during a reporting period. Incorporating benchmark data within dashboards and scorecards bring meaning and salience to actual-to-budget and variance reporting.
Business Analytics ñ A predictive process of the future derived via data mining exercises. The focus is gaining new perspectives about business processes. It involves the exploration of database contents for the purpose of gaining insight of future trends These techniques are statistical or quantitative; they may focus on new regulatory issues, changing financial incentives, new technology innovation. It employs data mining techniques, preferably from a comprehensive discharge abstract database that includes financial information, and statistical methods (frequencies/cross-tabs/clustering, etc). Healthcare Analytics are interpretive of that data.
Business Intelligence Using metrics to understand current operations. Focus is statistical tracking using compiled data from internal source systems. Metrics are included in dashboard and scorecard designs to enhance meaning of service volume and finances associated within discrete program parameters (e.g. cost center/department/service line). The algorithms or logic behind the metric have been created and agreed upon within the facility -- have been applied to software applications and now become integral to an organization's current statistical reporting.
As health insurers focus affordability and risk sharing with providers, competitive rates and controls play an significant role in remaining profitable. Data mining exercises focused upon disease specific episodes and practitioner behaviors are crucial profiling exercises in this new environment.

Case Mix Index ñ An indicator of the level of severity of the patients treated by a provider ñ and itís costliness as well! Typically a DRG type classification system containing relative service weights for each DRG type is used during grouper computation of the statistic. The relative weight is a dependant variable per the calculation of multiple diagnoses and procedures within that grouper software algorithm. Simply stated: the higher the service weight of a discharge -- the higher the reimbursement payment.
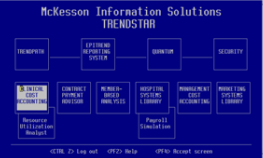
ChargeMaster -A register of all tests/orders/procedures that may be performed by the provider. It is commonly referred to as the price schedule of the provider. But from a Business Analytics perspective it is the repository of discrete clinical utilization activities and procedures performed during a patient care episode. The facility's internal Chargemaster is a proxy of clinical activities done by that provider. An example of a ChargeMaster. Further data mining exercises within a statistical context, such as a DRG assignment, can produce statistical information about clinical outcomes, treatment protocols, and payment trends for myriad segmented populations the facility is reviewing.
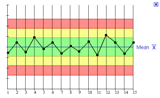
Control Chart - A visual display of processes. The time element is displayed on the horizontal axis and displays any variation over the time period. Well conceived Decision Support Systems can help drill down within those specific patient records and help locate the core reasons or narrow the reasons for the variation within those cases.
Cost Shifting ñ The commonly understood notion that provider costs incurred during an episode of care may be shifted/reallocated to payers with more generous payment rates to compensate for lost revenues. But there is less validity to this idea when studied. It has been advanced that there is usually but one cost and while there may be plural prices; it presents needless complexity (i.e. managing the ChargeMaster) for the facility. Cost shifting has been debunked by MedPac in testimony to Congress.
 Dashboard - A visual vehicle, usually a chart or table, demonstrating an organization's performance. It works best when it includes other measures (benchmarks) to contrast the current status -- to provide perspective about the actual performance data. The Dashboard aims to provide Business Intelligence to a wide spectrum audience. It shows the big picture and is intuitive. With data mining tools it drills down within the facility-wide metrics to locate core issues and problem areas.
Dashboard - A visual vehicle, usually a chart or table, demonstrating an organization's performance. It works best when it includes other measures (benchmarks) to contrast the current status -- to provide perspective about the actual performance data. The Dashboard aims to provide Business Intelligence to a wide spectrum audience. It shows the big picture and is intuitive. With data mining tools it drills down within the facility-wide metrics to locate core issues and problem areas.
Database ñ The organization of electronic information. Organized in a structured way, it permits a computer program to quickly select data elements (e.g. zip, Dx, carrier, etc) from records located in the file about the patient. In a hospital decision support system records are usually appended to a database post discharge.
Data Cleansingñ A data capture process that keeps data records accurate and up-to-date. The computer processing routine updates patient digital records with the most recent changes and modifications, thereby making Year-To-Date statistical reports more accurate than previous versions. A good illustration of data cleaning is that of a patient readmission but upon utilization review the care provided during this time frame is deemed a continuation of the previous admission rather than a new episode of care.
Data Mining ñ Transforming data to information. It is a structured inquiry process for gaining insight about a complex issue. It is about discovering new patterns within the data; of recognizing new relationships or correlations within a facility's data files and it's reporting' In high performing organizations it can lead to insights and root cause investigations about patient treatments and provider care patterns and trends. A convenient methodology is the creation of sub populations and reporting classifications that are repeatedly applied to updated databases yet leave the report qualifications intact for futre report productions. Data Mining exercises improve a facility's predictive behavior.
Disruptive Innovation - A transformational force in the marketplace. Innovation within an industry's traditional business model; introduces affordability and convenience to consumers. In healthcare this era is characterized by new payment methods, risk sharing arrangements, technology implementation and consumer satisfaction. Health insurance executives indicate initiatives to reduce insurance middleman overhead and engage providers to assume risk in manageing consumer\patient health. Current healthcare examples include: payment bundling, Medicare beneficiary ACO assignments, physician alignment, meaningful use IT implementation, patient survey reports.
Encounter ñ A patient event -- an episode of care. A single encounter is typically characterized as beginning with an Admit date and concluding with a Discharge date. Within these parameters, the patient record or data file record, contains diagnoses (principle, admit and/or working), procedures, physicians, orders and tests. Charge code items being a quick locator of such. It is these data elements in coded form (ICD-9, DRG, CDM) that are the building blocks for empirical analyses. With implementation of the 2010 Patient Protection and Affordability Act, providers can expect and even more detailed structure about an encounter. Payment claim forms may require the reporting of all patient services from Accountable Care Organizations to be included.
Essential Benefits - A basic benefit package (diagnostic, therapeutic and preventive) that every qualified health plan must include in any marketed plan. The criteria include (1) ambulatory care, (2) emergency services, (3) acute care, (4) lab services, (5) maternal care, (6) mental health care, (7) pediatric care, (8) wellness services and (9) rehab services and (10) prescription drug services. The statute covers emergency services without the need for pre-authorization. It covers preventive services and chronic disease management without cost sharing arrangements to the insured. It expands coverage for children up to age 26. No limit attached to annual spending or lifetime spending for defined essential benefits. Although the criteria have been indicated (items 1-10) the actual range of covered service within each of the criteria is subject to each state's designation as enrollments will rise in future years. Mandated coverage begins in 2014.
Level of Severity ñ An indication of how sick the patient is. Based on all medical chart indicated clinical conditions at time of discharge, that include and prioritize the principle diagnosis, it also accounts for comorbidities, all surgical procedures performed and the age of patient -- a classification of between 1 to 4 is rendered by this DRG grouper type software. This indicator provides an unbiased evaluation of the patient's medical condition. It is an important discreet variable for almost any quality or financial analyses and this metric should be extant in the discharge record within the data mining system to enable significant reporting.
Meaningful Use - The PPACA has numerous citations to the development the electronic health record (EHR) and meaningful uses implicit in it. Although the electronic health record (EHR) has often been expressed in daily parlance the PPACA has tightened their definition of an EHR. Medicare EHR certification standards include three aspects: (1) interoperability to share data with other systems, (2) have capability to store patient data and (3) the security of the system. Software vendors must apply for the distinction of software applications being EHR approved. Software certification awarded to vendors is managed by the Office of the National Coordinator for Health Information Technology (ONC) . But the validity behind meaningful use measurement remains to be determined by providers themselves. Applications to ONC for demonstrations showing meaningful EHR use by professionals and provider organizations begins in early 2011. Meaningful use benefits suggestions might include quality initiatives, engaging patients in their care regimens and lowering provider administrative costs.
Medical-Loss Ratio ñ The percentage of HMO premium revenues that pay for medical services. Originally an internal cost/revenue metric created by insurers, this indicator has acquired new salience as a result of the 2010 Patient Protection And Affordability Act (PPACA). It requires 85% of premiums in large group markets be spent on medical care and 80% in individual markets.
Recent observations (summer 2010) include an accounting definition brouhaha about insurer expenses that constitute patient care. Some insurers in the aftermath of the passed legislation had services, community education, case management are examples -- reclassified as patient care costs. The National Association of Insurance Commissioners (NAIC) is creating uniform definitions that would quality as patient care specific. With future regulatory implementation of the PPACA, Managed Care Organizations may begin behaving like regulated utilities. As the CMS regulations are being mandated, it will impact future care delivery. Should service types be excluded from the definitional mandates it (1) may impede the coordination of care delivery and (2) distort the planned creation of Accountable Care Organizations.
Medicare Payment Advisory Commission - ñ Advises the CMS and the U.S. Congress on issues of access to care, cost and quality affecting the operation of the Medicare program. Members of the commission are specialists versed in abstruse healthcare policy issues affecting payment, access, quality. MedPAC expertise has gained in stature; currently there exist proposals to bring this expertise within the executive branch of government and exert a even more substantive role in healthcare reform. The opinions expressed by its individual members are thought and extensively researched; they should frame facility strategic planning efforts.
Medical Underwriting - A risk assessment process by an insurer. During medical underwriting an insurer aims at locating conditions affecting the degree of future risk (costs) and adjusting premiums accordingly. It is a determination of risk associated with the medical characteristics of a person or demographics of a population. A review of medical status information by the insurer preclude an adverse selection process within the insurance pool. It also includes the expansion\limitation of practitioners within it's panel of providers.
Observation Days - An evaluation period during an inpatient hospital episode. It is usually a 24-48 hour observation period for a condition that can potentially be serious. It may lead to an initial diagnosis that is the basis for a hospital admission or a referral to other treatment options. Payment disputes revolve around the issue of whether it meets the Medical Necessity test.

Pay for Performance - Providers are rewarded for meeting agreed upon goals for the delivery of healthcare services. From an evaluation research vantage point a common database used by all hospital managers, rather than extracts created for quality or managed care staff is a more appropriate vehicle. Statistical counts will be less confusing and commonality minimizes administrative overhead of tracking performance. (ie Leapfrog Group, Institute of Medicine)
Performance Management ñ An empirically based approach to evaluating operational, clinical and financial segments of a provider. It employs program evaluation type methodologies to measuring results by benchmarking internal statistics against those of empirically based standards. No longer considered just an internal mechanism for improvement, indices published in the public record inform patients, insurers and employer groups of the organization's clinical and financial performances. As providers transition to more risk based reimbursement methods, providers can realize the rewards of their organizational improvements. In the current environment, benchmarking clinical performances is fundamental for improved financial ratios in the financial realm as well.

PPACA - Patient Protection and Affordability Care Act; signed March 23, 2010
Program Management ñ Is a broad stroke approach to managing a patient activity. It balances outputs (e.g. clinic visits/screening, etc) against the costs (e.g. personnel supply, etc) of a measured output. Program Management is ideally suited to data mining analyses because many of the outputs (tests/meds/orders) are measured somewhere in the facility and often, but not always, a provider has created a costing formula or algorithm to estimate the actual cost to the provider. All of these metrics are part and parcel of the patient discharge record and enhance the linking of quality with cost analyses.

Readmission - - A related admission to a hospital within 30 days. Readmissions indicate inferior care and poor focus on transitioning the patient upon discharge. It is regarded as a preventable event; as such governmental and private insurers are increasingly less willing to reimburse for such care. It is essentially a de facto continuation of that earlier hospital length of stay. Indeed MedPAC suggested in 2009 reducing payment to hospitals for select conditions with high readmission rates. Medicare has addressed this issue on several fronts: imposition of financial penalties for hospitals with high readmit rates beginning FY-2012 for discharges that are acute myocardial infarction, heart failure and pneumonia. Although unpopular within the hospital sector many notable teaching hospitals penalized in the first round of Medicare sanctions have improved their readmit rates for the 2014 fiscal year. Having a strong Home Health Program or a Post-Discharge Clinic in place is important. Preventable admissions might also be revealed via ACO claim submissions of those providers.
Reliability ñ The consistency of a data element for measurement. Represents confidence in using the statistic as a trusted measure of performance. An example of unreliability can be that of too quickly computing a monthly CMI -- as perhaps not all monthly discharges have yet to be abstracted. In the same manner, it is the principle diagnosis as defined by Health Information Professionals rather than the Admitting Dx or the Working Dx that clinical characterizes a discharge record and for which statistics are generated

Revenue Cycle Management ñ Administrative tasks associated with getting payment for services rendered. Process that begins with information gathering at registration before services are performed and is completed when a zero balances posting is computed in the patient account record. The cycle process includes obtaining demographic and insurance information. It includes verifying insurance eligibility, identifying the guarantor of payment, and obtaining medical necessity to forestall payment denial. It may include an assessment of ability to self-pay for whatever services are provided. Within the provider organization it may require updates and revisions to its chargemaster and related tables. A standard benchmark is to complete the account management process within 90 days.
Risk ñ The possibility of loss. For an insurer it is the payout caused by the estimated\negotiated costs associated with the delivery of patient care. For the provider reform legislation has ramped up the prospect of risk when delivering care services. Post discharge services are bundled in single payment reimbursements and quality issues (adverse events, readmission, etc) can nullify expected payment of the DRG based discharge
Root Cause Analysis ñ Discovering the core factor underlying a study issue. It is an empirically derived discovery process. Root Cause Analysis, while manipulating a database, is a top down data mining study approach aimed at locating core processes.
Special Care Days ñ Patient care days in intensive care units. It includes: intensive care unit days, coronary care unit, burn unit, total surgical intensive care unit, and other special care units. Just as a high CMI indicates a severity of illness, special care days is a metric providing insight about caseload characteristics and the severity of the medical management required of cases at the facility.
Survey Research - An empirical process to assess attitudes and opinions. Primary research like surveys lend credibility to the organizational strategies derived from provider transaction data files. Recent digital advances of merging discharge records with survey respondent data means that utilization data can be leveraged to more closely associate patient opinions and forecasts with outcomes and costs linked to specific service line performances.
SWOT ñ Issues surrounding the Accountable Care Act have dampened the validity of this approach per long range planning, as reform is focused on restructuring the single patient episode for every provider. Innovations like bundled payments and shared saving have obfuscated short term cost-revenue calculations as long term investments and experience in new delivery methods is paramount.
Table Driven ñ Data in a form suitable for ready reference. A software design feature that allows for quick changes in the application (e.g. billing rates, site locations, diagnosis codes, etc) but does not change the computer program routine for manipulating the data. It is standard feature of vendor purchased hospital applications. In this manner annual updates to ICD-9 diagnoses and procedures and CPT codes are unobtrusively updated.

Unit of Analysis ñ A degree of measurement: days, clinic visits, charge code items, patient types, discharge DRGs, ICD-9 diagnoses/procedures, consults, attending, surgeons, level of severity indicators, nursing units, payments, dates of payment, expected payment, adjustments, etc.
Utilization Review ñ A process to evaluate care provided and necessity. Chargemaster items and CPT code entries are prime elements for identifying care services rendered during an episode. The provider or insurer objective is to systemize the delivering of appropriate care while minimizing procedures, tests and other care orders of negligible benefit but never-the-less increase total medical costs
Value Based Purchasing - Reimbursement mechanism whereby hospital payments are linked to about two dozen quality performance measurements. During FY2014 there are more hospitals incurring penalties and incentives. For Medicare discharges clinical measures count for 70% and the patient experience for 30%. Hospitals will experience a 1% decrease in a DRG payment, but VBR based reimbursement serves as an incentive system to share an amount CMS estimates at $850 million to (1) improve the quality of care delivered and the(2) overall patient experience.
The recent inclusion of mortality rates into the CMS calculation speeds the momentum for sifting through discharge data by hospitals. Analyzing below average trends within service lines can locate root cause issues impacting reimbursements.
